




































Gonarthrosisit is deforming arthrosis of the knee joint. It is accompanied by damage to the hyaline cartilage of the articular surfaces of the tibia and femur and has a chronic progressive course. Clinical symptoms include pain that worsens with movement, limitation of movement, and synovitis (fluid accumulation) in the joint. In the later stages, support on the legs is damaged and a marked limitation of movements is observed. Pathology is diagnosed on the basis of anamnesis, complaints, physical examination and radiography of the joint. Treatment is conservative: drug therapy, physiotherapy, exercise therapy. If there is significant destruction of the joint, endoprosthetics are indicated.
General information
Gonarthrosis (from the Latin genus articulatio - knee joint) or deforming arthrosis of the knee joint is a progressive degenerative-dystrophic lesion of the intra-articular cartilage of a non-inflammatory nature. Gonarthrosis is the most common arthrosis. It usually affects middle-aged and elderly people, more often women are affected. After injury or continuous intense stress (for example, during professional sports), gonarthrosis can occur at a younger age. Prevention plays the most important role in preventing the occurrence and development of gonarthrosis.
Contrary to popular belief, the cause of the development of the disease does not lie in the deposition of salts, but in malnutrition and changes in the structure of intra-articular cartilage. With gonarthrosis, foci of calcium salt deposition may occur at the site of attachment of the tendon and ligamentous apparatus, but they are secondary and do not cause painful symptoms.
Causes of gonarthrosis
In most cases, it is impossible to identify any single reason for the development of pathology. As a rule, the appearance of gonarthrosis is caused by a combination of several factors, including:
- INJURY. Approximately 20-30% of gonarthrosis cases are associated with previous injuries: fractures of the tibia (especially intra-articular), meniscus injuries, tears or ruptures of ligaments. Typically, gonarthrosis occurs 3-5 years after a traumatic injury, although an earlier development of the disease is possible - 2-3 months after the injury.
- Physical exercises. Often the manifestation of gonarthrosis is accompanied by excessive loads on the joints. The age after 40 years is a period when many people realize that regular physical activity is necessary to keep the body in good condition. When they start exercising, they do not take into account age-related changes and unnecessarily load the joints, which leads to the rapid development of degenerative changes and the appearance of gonarthrosis symptoms. Running and intense fast squats are especially dangerous for the knee joints.
- Excess weight. With excess body weight, the load on the joints increases, both microtrauma and serious injuries (meniscal tears or ligament tears) occur more often. Gonarthrosis is especially difficult in obese patients with severe varicose veins.
The risk of gonarthrosis also increases after previous arthritis (psoriatic arthritis, reactive arthritis, rheumatoid arthritis, gouty arthritis or ankylosing spondylitis). In addition, risk factors for the development of gonarthrosis include genetically determined weakness of the ligamentous apparatus, metabolic disorders and impaired innervation in some neurological diseases, traumatic brain injuries and spinal cord injuries.
Pathogenesis
The knee joint is formed by the articular surfaces of two bones: the femur and the tibia. On the front surface of the joint is the patella, which, when moving, slides along the depression between the femoral condyles. The fibula does not participate in the formation of the knee joint. Its upper part is located laterally and just below the knee joint and connects to the tibia through a low-motion joint.
The articular surfaces of the tibia and femur, as well as the back surface of the patella, are covered with smooth hyaline cartilage, very strong and densely elastic 5-6 mm thick. Cartilage reduces frictional forces during movements and performs the function of shock absorption during shock loads.
In the first stage of gonarthrosis, blood circulation in the small intraosseous vessels that feed the hyaline cartilage is interrupted. The surface of the cartilage becomes dry and gradually loses its softness. Cracks appear on its surface. Instead of sliding smoothly and unhindered, the cartilage "sticks" to each other. Due to continuous microtraumas, cartilage tissue becomes thinner and loses its shock-absorbing properties.
In the second stage of gonarthrosis, compensatory changes occur in the bone structures. The common platform is flattened, adapting to increased loads. The subchondral area (the part of the bone immediately below the cartilage) thickens. Bone growths appear along the edges of the articular surfaces - osteophytes, which in their appearance on radiographs resemble thorns.
During gonarthrosis, the synovial membrane and joint capsule also degenerate and become "wrinkled". The nature of the joint fluid changes - it thickens, its viscosity increases, which leads to a deterioration of its lubricating and nutritional properties. Due to the lack of nutrients, cartilage degeneration is accelerated. The cartilage becomes even thinner and in some areas it disappears completely. After the cartilage disappears, the friction between the articular surfaces increases significantly and degenerative changes progress quickly.
In the third stage of gonarthrosis, the bones are significantly deformed and seem to be pressed against each other, significantly limiting movement in the joint. Cartilage tissue is practically absent.
Distribution
Considering the pathogenesis in traumatology and orthopedics, two types of gonarthrosis are distinguished: primary (idiopathic) and secondary gonarthrosis. Primary gonarthrosis occurs without previous trauma in elderly patients and is usually bilateral. Secondary gonarthrosis develops against the background of pathological changes (diseases, developmental disorders) or injuries of the knee joint. It can occur at any age, usually unilateral.
Considering the severity of pathological changes, three stages of gonarthrosis are distinguished:
- The first phase– initial manifestations of gonarthrosis. It is characterized by periodic dull pain, usually after a significant load on the joint. There may be a slight swelling of the joint that goes away on its own. There is no deformation.
- Second phase- increased symptoms of gonarthrosis. The pain becomes longer and stronger. A crackling sound often occurs. There is mild or moderate limitation of motion and mild joint deformity.
- The third stage- clinical manifestations of gonarthrosis reach their maximum. Pain is almost constant, walking is impaired. There is a marked limitation of mobility and visible deformity of the joint.
Symptoms of gonarthrosis
The disease begins gradually, gradually. In the first stage of gonarthrosis, patients experience minor pain when moving, especially when going up or down stairs. There may be a feeling of stiffness in the joints and "tightness" in the popliteal area. A characteristic symptom of gonarthrosis is "initial pain" - painful sensations that occur during the first steps after rising from a sitting position. When a patient with gonarthrosis "diverges", the pain decreases or disappears, and after considerable stress it appears again.
Externally the knee has not been changed. Sometimes patients with gonarthrosis notice a slight swelling of the affected area. In some cases, in the first stage of gonarthrosis, fluid accumulates in the joint - synovitis develops, which is characterized by an increase in the volume of the joint (it becomes swollen, spherical), a feeling of heaviness and limitation of movements.
In the second stage of gonarthrosis, the pain becomes stronger, appears even with light loads and intensifies with intensive or long walking. As a rule, the pain is localized along the inner front surface of the joint. After a long rest, painful sensations usually disappear and reappear with movement.
As gonarthrosis progresses, the range of motion in the joint gradually decreases, and when you try to bend the leg as much as possible, sharp pains appear. There may be a harsh screeching noise when moving. The node configuration changes, as if expanding. Synovitis occurs more often than in the first stage of gonarthrosis and is characterized by a more continuous course and accumulation of more fluids.
In the third stage of gonarthrosis, the pain becomes almost constant, disturbing patients not only while walking, but also at rest. In the evening, patients spend a long time trying to find a comfortable position to sleep. Often the pain appears even at night.
Bending at the joint is significantly limited. In some cases, not only bending, but also extension is limited, therefore the patient with gonarthrosis cannot fully straighten the leg. The joint is enlarged and deformed. Some patients experience hallux valgus or varus deformity - the legs become X or O-shaped. Due to the limited movements and deformation of the legs, the gait becomes unstable and wobbles. In severe cases, patients with gonarthrosis can only move with the help of a cane or crutches.
Diagnosing
The diagnosis of gonarthrosis is made on the basis of the patient's complaints, objective examination data and X-ray examination. During the examination of a patient with the first stage of gonarthrosis, external changes usually cannot be detected. In the second and third stages of gonarthrosis, the roughness of the bone contours, the deformation of the joint, the limitation of movements and the curvature of the axis of the limbs are observed. When the patella moves transversely, a cracking sound is heard. Palpation reveals a painful area from the inside of the patella, at the level of the joint space, as well as above and below it.
With synovitis, the joint increases in volume, its contours soften. A bulge is detected along the anterolateral surfaces of the joint and above the patella. By palpation, the fluctuation is determined.
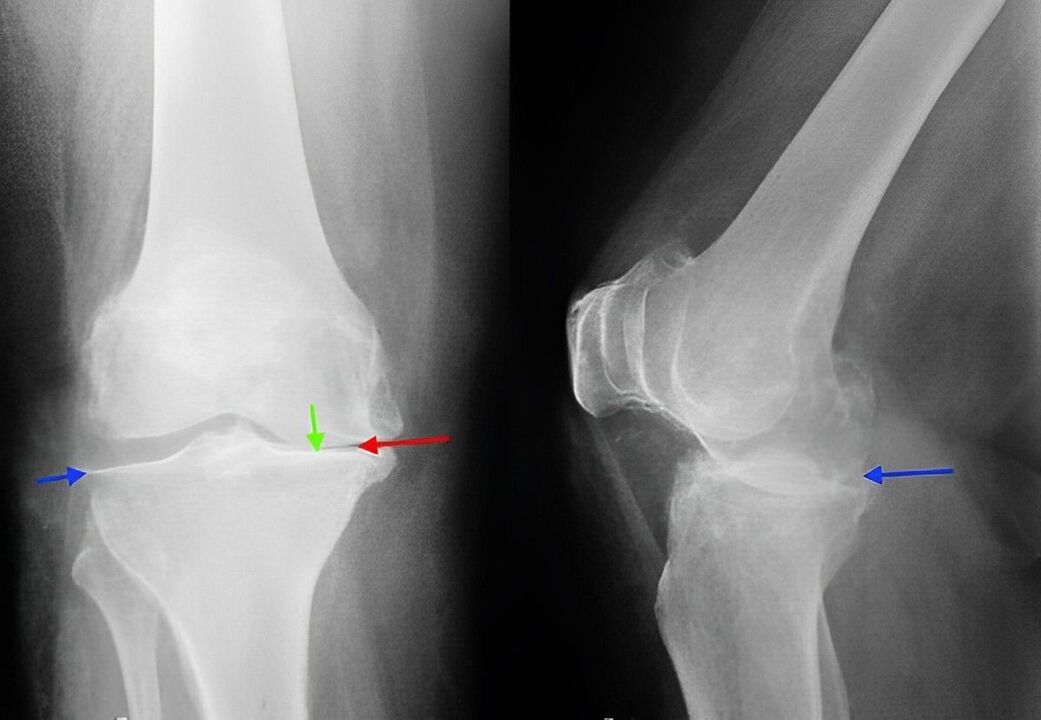
X-ray of the knee joint is a classic technique that allows you to clarify the diagnosis, determine the severity of pathological changes in gonarthrosis and monitor the dynamics of the process, taking repeated pictures after some time. Due to its availability and low cost, it remains the main method for diagnosing gonarthrosis to this day. Moreover, this research method allows us to exclude other pathological processes (for example, tumors) in the tibia and femur.
In the initial stage of gonarthrosis, radiographic changes may be absent. Then, a narrowing of the joint space and compression of the subchondral area is determined. The articular edges of the femur and especially the tibia widen, the edges of the condyle become sharp.
When studying radiography, it should be taken into account that the more or less marked changes characteristic of gonarthrosis are observed in most of the elderly and are not always accompanied by pathological symptoms. The diagnosis of gonarthrosis is made only with a combination of radiological and clinical signs of the disease.
Currently, along with traditional radiography, modern techniques such as computed tomography of the knee joint, which allows a detailed study of pathological changes in bone structures, and MRI of the knee joint, used to identify changes in the tissues ofsoft, are used to diagnose gonarthrosis. .
Treatment of gonarthrosis
Conservative activities
Treatment is carried out by traumatologists and orthopedists. Therapy for gonarthrosis should begin as soon as possible. During the period of deterioration, the patient with gonarthrosis is recommended to rest for maximum unloading of the joint. The patient is prescribed therapeutic exercises, massage, physiotherapy (UHF, electrophoresis with novocaine, phonophoresis with hydrocortisone, diadynamic current, magnetic and laser therapy) and mud therapy.
Drug therapy for gonarthrosis includes chondroprotectors (drugs that improve metabolic processes in the joints) and drugs that replace synovial fluid. In some cases, with gonatrosis, intra-articular administration of steroid hormones is indicated. Then, the patient can be referred for treatment at the sanatorium.
A patient with gonarthrosis may be advised to walk with a cane to unload the joint. Sometimes special orthotics or custom insoles are used. To slow down the degenerative processes in the joints with gonarthrosis, it is very important to follow some rules: exercise, avoid unnecessary stress on the joints, choose comfortable shoes, monitor your weight, properly organize your daily routine (alternate load and rest, performing special exercises).
Surgery
With pronounced destructive changes (in the third stage of gonarthrosis), conservative treatment is ineffective. In cases of severe pain, joint dysfunction and limited ability to work, especially if a young or middle-aged patient suffers from gonarthrosis, they turn to surgery (knee replacement). Then, rehabilitation measures are carried out. The full recovery period after joint replacement surgery for gonarthrosis lasts from 3 months to six months.