



































Osteoarthritis of the shouldersChronic is chronic a disease in which articular cartilage tissue is destroyed and thinned, pathological changes occur in the soft tissues and bone growths form in the joint area. It manifests itself with pain and pressure in the affected area. In the later stages, the range of motion decreases. The pathology is chronic and gradually progresses. Diagnosis is made taking into account the clinical appearance and radiological signs. Treatment is usually conservative: physiotherapy, anti-inflammatory drugs, chondroprotectors, exercise therapy. When the joint is destroyed, arthroplasty is performed.
a disease in which articular cartilage tissue is destroyed and thinned, pathological changes occur in the soft tissues and bone growths form in the joint area. It manifests itself with pain and pressure in the affected area. In the later stages, the range of motion decreases. The pathology is chronic and gradually progresses. Diagnosis is made taking into account the clinical appearance and radiological signs. Treatment is usually conservative: physiotherapy, anti-inflammatory drugs, chondroprotectors, exercise therapy. When the joint is destroyed, arthroplasty is performed.
General information
Osteoarthritis of the shoulder joint is a chronic disease in which, as a result of degenerative-dystrophic processes, cartilage and other joint tissues are gradually destroyed. Osteoarthritis usually affects people aged 45 and over, but in some cases (after injury, inflammation), the disease can develop at a younger age. Pathology equally often occurs in women and men, more often observed in athletes and people involved in hard physical work.
reason
The starting point for changes in osteoarthritis of the shoulder joint can be as the normal process of tissue aging and damage or disruption of cartilage structure as a result of mechanical influences and various pathological processes. Primary osteoarthritis is usually detected in the elderly, secondary (developed against the background of other diseases) can occur at any age. The main reasons are considered:
- Developmental defects.Pathology can be detected with underdevelopment of the humerus or glenoid cavity, shoulder capellarity, and other upper limb abnormalities.
- Traumatic injury.Osteoarthritis of traumatic etiology most often occurs after intra-articular fractures. A possible cause of the disease may be shoulder dislocation, especially the common one. Less often, severe bruising acts as a provocative injury.
- Inflammatory processes.The disease can be diagnosed with long-term shoulder-shoulder periarthritis, previously suffering from nonspecific purulent arthritis and specific ankle arthritis (with tuberculosis, syphilis and some other diseases).
Risk factors
Arthrosis is a polyetiological disease. There is a wide range of factors that increase the likelihood of this pathology:
- Hereditary predisposition.Many patients have close relatives who also suffer from osteoarthritis, including those of other localizations (gonarthrosis, coxarthrosis, ankle arthrosis).
- Joint overload.It can occur in volleyball players, tennis players, basketball players, throwers of sports equipment, as well as in people whose profession involves a constant high load on their hands (hammer, loader).
- Other pathologies.Osteoarthritis is most often detected in patients suffering from autoimmune (rheumatoid arthritis), some endocrine diseases and metabolic disorders, systemic connective tissue insufficiency and excessive joint mobility.
The likelihood of developing the disease increases dramatically with age. Frequent hypothermia and adverse environmental conditions have a certain negative impact.
Pathogenesis
The main reason for the development of osteoarthritis of the shoulder joint is a change in the structure of the articular cartilage. Cartilage loses its softness and elasticity, sliding of articular surfaces during movement becomes difficult. Microtrauma occurs, which leads to further deterioration of cartilage tissue condition. Small pieces of cartilage detach from the surface, forming elongated articular bodies, which also damage the inner surface of the joint.
Over time, the capsule and synovium thicken, showing areas of fibrous degeneration. Due to the thinning and reduced elasticity, the cartilage ceases to provide the necessary shock absorption, therefore, the load on the underlying bone increases. The bone deforms and grows along the edges. Normal node configuration is interrupted, there are movement restrictions.
Distribution
In traumatology and orthopedics, a three-stage systematization is commonly used, reflecting the severity of pathological changes and the symptoms of osteoarthritis of the shoulder joint. This approach allows you to choose the optimal medical tactics, taking into account the severity of the process. The following stages are distinguished:
- First- no gross changes in cartilage tissue. The composition of synovial fluid is altered, cartilage nutrition is impaired. Cartilage does not tolerate stress, therefore, joint pain (arthralgia) occurs occasionally.
- Second- cartilage tissue begins to thin, its structure changes, the surface loses its softness, cysts and calcification areas appear in the depths of the cartilage. The underlying bone is slightly deformed, bone growths appearing along the edges of the articular platform. The pain becomes permanent.
- The third- marked thinning and deterioration of the cartilage structure with extensive areas of destruction. The articular platform is deformed. Detected limitation of range of motion, weakness of the ligament apparatus, and atrophy of the periarticular muscles.
Symptoms
In the early stages, patients with osteoarthritis worry about minor discomfort or pain in the shoulder joint during exercise and certain body positions. Crunching can occur during movement. The joint is not changed from the outside, there is no edema. Then the intensity of pain increases, arthralgias become common, constant, appear not only during exercise, but also at rest, including at night. Distinctive features of pain syndrome:
- Many patients notice the dependence of pain syndrome on weather conditions.
- Along with aching pain, over time, there is a sharp bitterness during physical exertion.
- The pain can occur only in the shoulder joint, radiate to the elbow joint or spread throughout the arm. Possible back and neck pain on the affected side.
After a while, patients begin to notice a noticeable morning stiffness in the joints. The range of motion decreases. After exercise or hypothermia, slight soft tissue swelling is possible. With the progression of osteoarthritis, movements are increasingly restricted, contractures develop, and limb function is severely impaired.
Diagnosing
Diagnosis is made by an orthopedic surgeon taking into account the characteristic clinical and radiological signs of osteoarthritis of the shoulder joint. If you suspect secondary osteoarthritis, consult a surgeon, endocrinologist. At first, the joint does not change, later sometimes it deforms or expands. By touch, pain is defined. Movement restriction can be detected. To confirm osteoarthritis, the following are recommended:
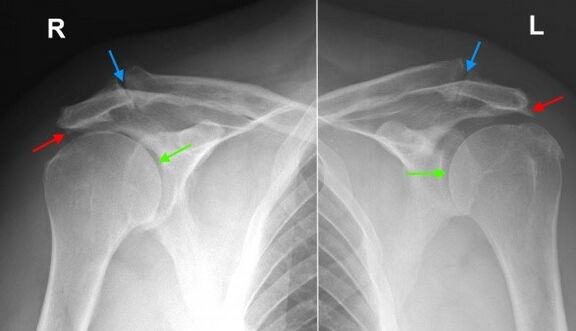
- Shoulder radiograph.Dystrophic changes and marginal bone growth (osteophytes) are found, in the later stages the narrowing of the joint space, deformation and changes in the structure of the underlying bone are determined. The joint gap may take a wedge-shaped shape, osteosclerotic changes and cystic formations are visible in the bone.
- Tomographic research.In suspicious cases, especially in the early stages of the disease, CT of the shoulder joint is performed to obtain additional data on the condition of the bones and cartilage. If it is necessary to assess the condition of the soft tissue, magnetic resonance imaging is performed.
Differential diagnosis
Differential diagnosis of osteoarthritis is made with gouty, psoriatic, rheumatoid and reactive arthritis, as well as with pyrophosphate arthropathy. With arthritis, a blood test shows signs of inflammation; changes in radiography are not very pronounced, osteophytes are absent, there are no signs of deformation of articular surfaces.
In psoriatic arthritis, along with articular manifestations, skin rashes are often found. In rheumatoid arthritis, a positive rheumatoid factor is determined. With pyrophosphate arthropathy and gouty arthritis, the biochemical blood test detects the corresponding changes (an increase in the level of uric acid salts, etc. ).
Treatment of shoulder osteoarthritis
Patients are under the supervision of an orthopedic surgeon. It is necessary to limit the load on the arm, excluding sudden movements, lifting and prolonged holding of weights. At the same time, it should be borne in mind that inaction also negatively affects the diseased joint. To keep the muscles in a normal state, as well as to restore the shoulder joint, you should regularly perform the complex of exercise therapy recommended by the doctor.
Conservative treatment
One of the most urgent tasks in osteoarthritis is the fight against pain. To eliminate pain and reduce inflammation, the following are described:
- General action drugs.NSAIDs are prescribed in tablets during an exacerbation. With uncontrolled use, they can irritate the stomach wall, have a negative effect on the condition of the liver and metabolism in cartilage tissues, therefore, they are taken only as instructed by a doctor.
- Local remedies.NSAIDs are commonly used in the form of gels and oils. Self-administration is possible if symptoms arise or intensify. Rarely, topical hormone preparations are indicated, which should be applied in accordance with the doctor's recommendations.
- Hormones for administration within the article.In case of severe pain syndrome, which can not be eliminated by other methods, intra-articular administration of drugs (triamcinolone, hydrocortisone, etc. ) is performed. Blockades are performed no more than 4 times a year.
To restore and strengthen cartilage in stages 1 and 2 of osteoarthritis, agents from the group of chondroprotectors are used - drugs containing hyaluronic acid, chondroitin sulfate and glucosamine. The courses of treatment are long (from 6 months to a year or more), the effect becomes noticeable after 3 or more months.
Physiotherapy treatment
With osteoarthritis of the shoulder joints, massage, physiotherapy exercises and physiotherapy techniques are actively used. During the remission period, patients are referred for spa treatment. Apply:
- mud and paraffin therapy;
- medicinal bath;
- magnetotherapy and infrared laser therapy;
- ultrasound
Surgery
In stage 3 of the disease, with significant cartilage destruction, limited mobility, and disability, joint replacement is performed. Reference for surgery is given taking into account the age of the patient, his level of activity, the presence of severe chronic diseases. The use of modern ceramic, plastic and metal endoprostheses allows you to completely restore the function of the joint. The service life of dentures is 15 years or more.
prediction
Arthrosis is a long-term, progressive disease. It can not be completely cured, however it is possible to significantly slow down the development of pathological changes in the joint, to maintain the ability to work and a high quality of life. To achieve the maximum effect, the patient must be serious about his illness and his willingness to follow the doctor's recommendations, even during the remission period.
Prophylaxis
Preventive measures include reducing household injuries, observing safety at work, eliminating excessive loads on the shoulder joint when performing professional tasks and when playing sports. It is necessary to diagnose and treat in time the pathologies that can provoke the development of arthritic changes.